Medical Emergency mid-Atlantic for Challenger 2
9,458 views | December 10th, 2017
You haven’t heard much from the FCS crew on Challenger 2 over the past few days and there has been a very good reason, one of the team was ill, seriously ill and this gripping account from skipper Ricky Chalmers will certainly have you on the edge of your seat…
Sunday December 10 2017 – Sailing to St Lucia
It’s been a while since the skipper or the crew of Challenger 2 have written a blog. That’s not to say that we didn’t have leaping dolphins, shooting stars or success at bread baking. No the daily routine of racing a yacht across the Atlantic continued on board Challenger 2 as it no doubt did on board hundreds of yachts taking part in this years ARC race/rally. We weren’t writing blogs, sharing out experiences with the outside world because we had a self imposed (well skipper imposed) clampdown on communications while we dealt with an ongoing medical emergency.
Four days out of the Cape Verdes and most of the crew were on deck enjoying the fresh air and the sunshine. Another pod of dolphins gracefully leapt along, pausing to play at out bow for a while and then moving on to find other playmates or to go and catch fish. Some of the crew were turning a golden brown in the baking, others who had been a bit less methodical with their application of sun cream were turning various shades of pink and red. By the end of the day, most were glowing and there was a general lethargy on deck coming from the days exertions of sunning themselves. We hadn’t seen seals on a beach yet, but the crew had collectively been doing a good impression…
One crew member was particularly out of sorts though and not his jovial self. He complained of not feeling very well. Feeling a tad sunburnt myself and knowing that I was a little dehydrated, I berated him for not covering up from the sun more, and for not drinking enough. Especially when he seemed shocked by being told that he should be drinking at least 2 litres of water/weak squash a day. Iona, one of the watch leaders, who is a doctor in her day job, took a more practical line of making up some rehydration salts and watching over whilst he drank them.
We were concerned. But only mildly so, more annoyed that all our warnings of drinking enough and using sun cream seem to have not prevented one of our crew suffering from an excess of the days rays.
Something More Serious that Sunburn
By morning it became clear that we were mis diagnosing the problem. Iona spotted the swelling of his right ankle and to her trained eye, this was not dehydration or sunburn – it was Cellulitis an infection of the soft tissue. The trusty “Ships Captains Medical Guide” has scant guidance for an infection which I was to discover is quite common and potentially very serious, even life threatening. Alarming initially that it is to be found in Chapter 6, Communicative Diseases.
Cellulitis (Erysipelas)
French: Erysipèle German: Erysipel Italian: Erisipela Spanish: Erisipela
Incubation Period:1 to 7 days
Period of communicability: None
Isolation Period: None
Quarantine Period: None
This disease is an acute inflammatory condition of the skin caused by a germ entering the body through a scratch or abrasion. Cellulitis occurs anywhere, but most commonly on the legs, arms and face. The onset is sudden with shivering, and a general feeling of malaise. The temperature rises rapidly and may reach about 40oC. The affected area becomes acutely inflamed and red on the first or second day of the infection and the inflammation spreads rapidly outwards with a well-marked, raised, and advancing edge. As the disease advances the portions of the skin first attacked become less inflamed and exhibit a yellowish appearance. Blisters may appear on the inflamed area which can be very painful.
General treatment
The patient must be kept in bed during the acute stage.
Specific treatment
Give the patient benzyl penicillin 600 mg followed by oral antibiotic treatment. Paracetamol can be given to ease the pain.
No not communicable – can’t be spread from crew mate to crew mate. We had a doctor on board – a bonus and we had recovered after stumbling at the first hurdle, we knew what we were dealing with. The diagnosis notched its credibility up considerably when Steve revealed that he had suffered this before earlier in the year. It had been simply treated before as an outpatient in a local clinic. A quick and simple course of antibiotics had dealt with the infection and his life had continued largely unaffected. Unfortunately now the nearest outpatient clinic was more than 800nm away at least five days sailing.

Dr Iona Taylor – the doctor on board
How to Get Medical Assistance mid-Atlantic
There is a well-established and highly effective means of getting medical assistance whilst at sea. Well I say assistance, really you get medical advice. The assistance you have to provide. You are the out patient clinic. You are the nurse, the doctor, the scribe and the medical orderly.
Your equipment is limited to what you have on board and your expertise is limited by who you have on board. In most cases, and in almost all ocean crossings that I have done in the past, this expertise consists of a two week “Medical Care Aboard Ship” course. Mostly done in a class room and mostly been made to feel slightly unwell by being shown slides of casualties in various gory states of disrepair.
In this case however we had hit the jackpot. We had a fully qualified medical doctor on board. She had come to race the ARC Rally 2017 across the Atlantic. She would find herself having to adapt her expectations of equipment and stability of the treatment facility to life on board Challenger 2.
The medical advice we got both from the UK coastguard and medical support provided by Queen Alexandria Hospital in Portsmouth and the CCMM French Medical organisation supporting the MRCC Fort De France local coast guard was very clear… IMMEDIATE EVACUATION FROM THE VESSEL.
Easy to write in an email, but when you are about as far from land as you can be in the North Atlantic, it is much harder to achieve. We were also to start Intravenous (IV) Treatment using Benzylpenicillin. Easy to achieve in a fully stocked hospital sterile treatment room. Not so simple in a 72 foot steel yacht trying to make best possible speed to the closest point of medical evacuation.
The challenger yachts and all Category zero coded commercial vessels carry a comprehensive medical kit called a Cat A med kit. This contains all the drugs with the unpronounceable names which we learn about in the Medical Card Aboard Ship course and all the tools of the trade, catheters, cannulas, needles and syringes. Knowing the difference between a cannula and a catheter can be important.
It holds a bewildering array of medicines, but they cover a vast array of things which can go wrong with the human body. Splints, staple guns and catheters are no good for putting in an IV line to administer drugs intravenously.
You need cannulas, bags of saline IV Fluid, green needles, syringes, dressings, anti-septic wipes, special water for making up the medicine and a lot of skill. You also would prefer a stable, non bumpy treatment room. Turns out we had the range of equipment but not the depth, not much of each.
You can use the same trusty slightly rusty sail repair needle over and over again as you repair your sails. Turns out it is frowned upon to reuse most medical equipment. Those green needles, those cannulas can only be used once then they get put in a “sharps box” – fancy medical term for Tupperware. Turns out you can’t use water fresh and drinkable made by the water maker to inject into patients. You have to use tiny glass vials labelled “water for injection” and having a blue dot on the vial to show you where to break the top off. Turns out we didn’t carry a lot of them. And we were going to need a lot.
Clear Thinking and Where to Go Next?
The Local coastguard Rescue coordination centre, MRCC Fort De France based in Antigua advised us that there could be no rescue within 48 hours. After that a rescue to a commercial ship was possible or we would have to divert to the nearest port of within 100nm of Martinique for a daytime only helicopter rescue. I considered the diversion options, scouring the electronic charts for nearest points of refuge. I breathed a sigh of relief, at least going back to the Cape Verdes for the third time was not an option, there were closer points.
- Gybe and head South West (course 200T for 48 hours) to French Guyana (Le Cheval Blanc). After 48 hours we would be approx. 340Nm off at approx. position 08 d 19 m North 047 d 39 m West
- Continue West to St Lucia, and get evacuation from Martinique or St Lucia or any other suitable island nearby.
- Divert to Bridgetown or Port St Charles, Barbados. Minor course adjustment. Course 265 T. We are currently 840Nm off Barbados, 100nm closer than St Lucia. After 48 hours we will be in approx. 13 d 28 North 51 d 25 m West, about 470nm off of Barbados.
- Come closer to wind by 15 degrees on a course of about 290T, get an extra 2 knots estimated. We are currently 1000nm away from Guadeloupe and after 48 hours assuming 9 knots of boat speed we will be in approx. position 15 d 41 m North 52 d 30 m West. That will put us about 520nm from Guadeloupe, Antigua or any of the higher islands.
Only the option of heading South South West to French Guyana required a radical course adjustment. The other options we could finalise as we continued heading West to the Caribbean island chain. The crew breathed a sigh of relief as I ruled out diverting to French Guyana. They would get to see the Caribbean after all…
The Yacht as a Treatment Room
We started to settle into a routine, A very different routine from before. With the saloon transformed into a treatment room and a massive schedule of email updates required to keep everyone informed.
My role in the treatment of Steve was limited, Iona managing to practice good medicine in the most testing of environments, I just popped open the little glass “water for injections” vials which turned out the be Iona’s Achilles heel and to then retire upstairs to take the helm and try introduce some stability and calmness in the boat while needles and cannulas were deployed.
Gary, the mate got to play a more hands on role, operating the tourniquet. We didn’t have a proper medically approved one in the Cat A medical kit – a trusty sail tie did the job, especially when operated by a northerner from Sunderland.
The realisation soon dawned on Iona that we were going through meagre supplies rapidly and that we would not be able to complete the treatment before she ran out. Simple stuff really, which you could pop down to the pharmacy for – except we couldn’t. We would run out of green needles, saline IV solution, possibly cannulas antiseptic wipes, fixing tape and syringes. The fixing tape wasn’t a big issue – we had a big roll of gaffer tape on board. The other bits were trickier.
In Search of a Floating Pharmacy
I did the sums, we were going to run out of essential medical supplies in two days and we were at least five days from a rescue. The coastguard had since ruled out a commercial or military ship evacuation, none were in our vicinity.
We needed to go shopping, quickly. The only shops around were the other 192 boats taking part in the 2017 ARC. One of them may have the kit we desperately needed. Time to “google” the shops and fine the best one. The ARC Rally Control team were fantastic in putting out the message requesting medical stores on our behalf. We were flooded with offers of help. How to choose the right store…
I ruled out anyone kind enough to offer assistance who didn’t have the stuff we needed. This wasn’t the time for impulse buys. We had a shopping list and we needed to stick to it. Also I considered that there was no point in turning around to supply from a boat behind us.
We were still trying to sail as fast as we could to a helicopter rendezvous point. Turning back even 50nm would cost an unacceptable number of hours. Risk management was time management. We needed to stay sailing fast in the right direction and still do our shopping.
An then the wonderful Talulah Ruby replied to us concerning the ARC request for medical stores on our behalf. They had everything – except the tourniquet. Not a deal breaker, the sail tie operated by the Northerner seemed to be working so far.
They were 120nm ahead of us and almost on the same Latitude, almost ahead of us on the course we were currently on to the Heli RV waypoint. Like finding that Frozen Yoghurt shop at the motorway services – perfect.
I emailed them and they couldn’t have been more helpful. Thank you Rebecca of Talulah Ruby. You may have a tongue twister of a boat name to say 3x on the VHF radio, but you were the perfect pharmacy shop in the perfect place at the perfect time. We just had to hunt you down and catch up the 120nm.
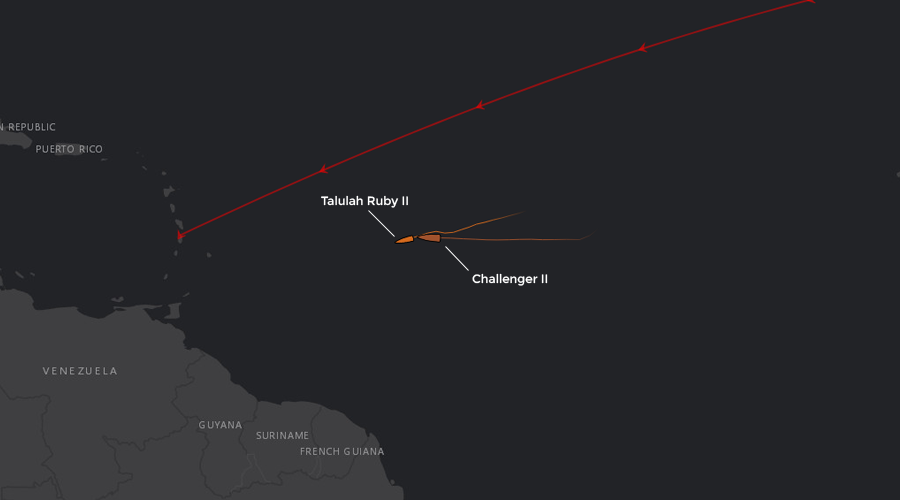
Position of both ships on Thursday 7th Dec 11:03 UTC
Full Speed to a Gem Called Talulah Ruby
When you are going 12 knots, 120nm is a short distance, only some ten hours away. But Talulah Ruby were also sailing. Also had places to get to, the ARC to finish. They slowed down for me by deep reefing their furling mainsail, but ultimately in 20 knots of downwind sailing they were still doing 7 knots.
We needed to sail faster… And so started a mad dash through the night. Boat speeds topped out at 14.5 knots and we enjoyed one of the best nights sailing. Well I did, I was keeping the treatment room as stable as possible. Iona was battling with failed cannulas and a dwindling stock of everything.
Eventually something had to run out, and it was the IV saline solution. Once that was finished she couldn’t flush the cannula or administer the benzylpennicillin no matter how many glass vials I popped open for her.
Treatment on Steve had to be suspended and the entire focus of the boat was on catching Talulah Ruby and doing the at sea resupply. That had to go smoothly and quickly but most importantly successfully. Without those stores, we couldn’t treat Steve and we were still three days from the nearest Helicopter range.
I laid out the plan for the resupply operating in great detail…there was no room for errors.
Boat Transfer Protocol
What follows is the boat to boat transfer procedure which I would like to use. Please come back if anything is unclear or if there is anything which you are unhappy about. I have done a number of boat to boat transfers in various oceans in the past and this procedure seems to be the safest and simplest.
Communications : VHF Channel 72
Please let me know if you have any major Compass Deviation
I understand from your AIS details that you are a 22 meter sailing vessel
We are a 21.5 meter sailing vessel
If you could get your vessel on a comfortable course, sailing if you are still racing or motor sailing if you are cruising and would presser that. Given the wind angles and sea state, I would recommend a broad reach with an apparent wind angle of about 120 degrees. Whatever boat speed you are comfortable with, but preferably more than 3 knots and less than 6. You want good steerage in the sea state but I need to be able control my approach and not be at max revs.
Once you are on course and feel you are able to maintain the course and speed, let me know on the VHF and tell me your Magnetic Compass Course and Speed Over Ground.
Please keep your course and speed as best as you can during the whole procedure. Please let me know if for any reason you have to alter course or if your speed changes radically. If you are sailing I will expect some minor ups and downs in speed especially as we have a swell.
I will approach your vessel on your windward side (Starboard side most likely in the conditions we have today). I will have headsails down and mainsail as appropriate for the conditions. I will be under engine.
We will have two large roving fenders manned by two crew members on the foredeck. They will be wearing life jackets and be clipped on. In addition to them on the bow, I will have my mate, Gary at the pulpit with the heaving line and another crew member sat on the port side with the container.
The heaving line is a 8mm throwing line with a monkeys fist tied in the one end. It is not weighted apart from the weight of the rope. The container will be a bright yellow plastic box with a screw top red lid, normally used to contain flares.
We will have an AIS Personal Locator beacon strapped to the container and active. You may receive that signal as an alarm on your AIS system.
I will overlap my port bow on your starboard stern quarter by about 6 meters. I will aim to be about 6 meters from your vessel. At a suitable moment, Gary will throw the heaving line aiming to throw the monkeys fist over your vessel. He will not aim at any one on your vessel. Please make your crew aware though of the potential danger of being hit by the monkeys fist.
Once you have retrieved the line and made an appropriate signal to Gary (a thumbs up or Divers OK sign will be sufficient), please secure the line to your vessel, a simple half hitch will suffice. Start pulling in the line onto your vessel. It is not especially important to keep the line taught we will pay out lots of slack. At the point that the line is almost fully paid out and has been pulled in to your boat, we will drop the container over the side of our vessel into the water.
At that point there will be a big increase in the resistance and pull on the line. Please could your crew be ready for that. I recommend that they wear sailing gloves. At that point I will reduce revs and we will drop back off your starboard quarter.
Please continue to pull the container on board. You shouldn’t need to untie the heaving line from the container. Please be aware that the AIS locator beacon has a whiplash sprung steel aerial which can scratch and potentially injure a crew member. Please unscrew the lid. We will have placed some items and some soft packing material in the box. Please remove the items and use the packing material to pad out the box.
If you could pack the container with the medical supplies you are providing us, and then pad it out with the packing material. Then secure the lid firmly. There is no need to rush this process. I will be behind your vessel about 2 boat lengths away on your leeward side. This will likely be on your port side.
If you could make up the heaving line as a throwing line by making up coils and splitting them into two sections. The thrower will throw the monkeys fist and about 3 coils of rope with his lead hand and follow with four or five coils of rope with his following hand. Please could you ensure that this person is clipped on to your vessel he will need to be standing on the Port side which will be the low side of the vessel. Please do not tie the heaving line to your vessel.
When everything is ready, please could you call on VHF channel 72 again to let me know and again confirm your Compass Course and Speed Over Ground.
I will approach your vessel on your Leeward Side (Port side), and will overlap your stern with my bow by about 6 meters. I will aim to be 4 to 6 meters from your vessel. At a suitable time. Please could your throwing person heave the line onto our foredeck. Aim to get the line over our guard wires. We have a high freeboard and will be heeled over away from you so they will need to throw high.
If they miss, I will drop back allowing you to retrieve the line and have another go.
When the line hits our foredeck, Gary will secure an end and start to pull the line on board our vessel. When he has almost all the line, please drop the container into the water. At that point I will reduce revs and we will drop back from your vessel and will recover the container.
As you are the stand on vessel and are going to be maintaining course and speed, I will take all responsibility for the manoeuvre.
The Moment Arrives
We finally spotted Talullah Ruby two hours before sunset under a squally dark sky with a very rolly sea. Not ideal, but we needed to press on, night time was not going to make it any easier. We charged up behind Talluah Ruby doing 13 knots of surfing with full main out on a preventer, staysail and Yankee 1 polled out.
It must have been an awesome sight and perhaps a bit intimidating and the prospect of a close quarter manoeuvre with us must have sent shivers down their spines. I think they breathed a sigh of relief as I asked them over the VHF to give us a minute to change our sail plan to something more suitable for the transfer.
What followed was a slick set of sail changes which made a stressed skipper very proud of his crew. Staysail down, and rolled away on the foredeck – check. Polled out Yankee across to leeward and down – check. Pole down – no jousting today – check. 2 reefs in the main, and pinned in – check. Engine on – check. Just like that we were good to go, and just as well – the light was fading fast as the last of the sun had slipped behind big black ominous clouds.
There is not much to say about the transfer except – perfect. I have watched back a couple of crew videos of the procedure and it went like clockwork. So so happy and relieved.
Thanks for the Chocolate – a Spoon Full of Sugar!
Pretty soon we were powered up with full sail and intent on making our Heli RV waypoint as soon as we could. Iona was all smiles as she opened the shopping bag and pulled out the long awaited goodies.
The bonus of chocolates from Talulah Ruby could wait – that IV drip needed to get going so the overdue treatment could be administered. I could stay on deck, “keeping a stable outpatient room” whilst just revelling in the lovely sailing conditions. 25 knots of wind, threatening skies and a supercharged sailing machine with full sail powering through waves at 13 knots.
With our new stock of medical supplies and now 48 hours into the treatment Steve finally started responding to the treatment. “hot and angry” turned into “warm and flushed” in the medical notes. The coloured lines being drawn on Steve’s leg in daily colour coded marker pens started shrinking in size. The smile and cheerful nature of the Steve we knew returned.
As we approached the Heli RV point to within 100nm of Martinique a conference call between myself, Iona, the MRCC coastguard and the CCMM medical team in Tollouse, France and translated for us by Leaticia concluded that Steve was now so much improved that the Helicopter ride was no longer needed, he would just have to enjoy the sailing all the way to St Lucia.
We have 132 miles to go and should reach or final goal of Rodney Bay, St Lucia later this afternoon. There hasn’t been a lot of sleep or downtime in the past few weeks. There has been a lot of stress on board and a lot of support given to us by the ARC Rally control team, Tall Ships, First Class Sailing, the French Coastguard and Medical Support team and not least by our shop in the sea, Talulah Ruby.
The story ends well but I wish for a less eventful crossing in ARC 2018 next year…
Kind regards
Ricky Chalmers, Skipper, Challenger 2

Ricky Chalmers, Skipper, Challenger 2
Posted by: First Class Sailing